Introduction
Emergency practitioners and other clinicians working in acute care settings frequently encounter patients who have trauma to or pathology of the dorsum of the foot and require anesthesia for treatment and repair.
Regional block of the superficial peroneal nerve allows for rapid anesthetization of the dorsum of the foot, which allows for management of lacerations, fractures, nail bed injuries, or other pathology involving the dorsum of the foot. Regional blocks have several advantages compared to local infiltration, such as fewer injections required to attain adequate anesthesia, smaller volume of anesthetic required, and less distortion of the wound site. Because of the lower number of injections, this procedure is better tolerated by the patient and limits the chance of a needle stick injury to the provider.
This procedure, often overlooked in the emergency department, is safe, is relatively easy to perform, and can provide excellent anesthesia to the foot. In one study, regional anesthesia of the foot and ankle, when performed by surgeons, was completely successful 95% of the time.
Anatomy
Understanding the anatomical distribution of the superficial peroneal nerve is helpful in performing a successful blockade of this nerve. The superficial peroneal nerve arises from the common peroneal nerve, which also gives rise to the deep peroneal nerve. The superficial peroneal nerve originates between the peroneus longus muscle and the fibula. It courses down the lateral compartment of the lower leg along with the peroneus longus muscle and the peroneus brevis muscle. It then descends posterolaterally to the anterior crural intermuscular septum. It runs anterolateral to the fibula between the peroneal muscles and the extensor digitorum longus, eventually supplying the peroneal muscles.
In the distal third of the leg, it pierces the deep fascia to become superficial. The nerve splits into the medial dorsal cutaneous nerve and the intermediate dorsal cutaneous nerve, which give rise to the dorsal digital nerves. These nerves supply the skin of the anterolateral distal third of the leg, most of the dorsal foot, and the digits. However, this nerve does not supply the web space between the first and second digits or the lateral fifth digit. At the level of ankle, the superficial peroneal nerve splits to fan out between the medial and lateral malleoli.

Dermatome of the superficial peroneal nerve at the level of posterior calf.

Superficial peroneal nerve dermatome at the level of the anterior lower leg.
Indications
- Wound repair or exploration of the dorsal regions of the foot
- As part of an ankle block required to manipulate a fracture or dislocated ankle (A combination of posterior tibial, saphenous, superficial peroneal, deep peroneal, and sural nerve blocks results in complete block of sensory perception beneath the ankle. Compared with more proximal approaches to the ankle block, motor block is rarely a concern with the ankle block.
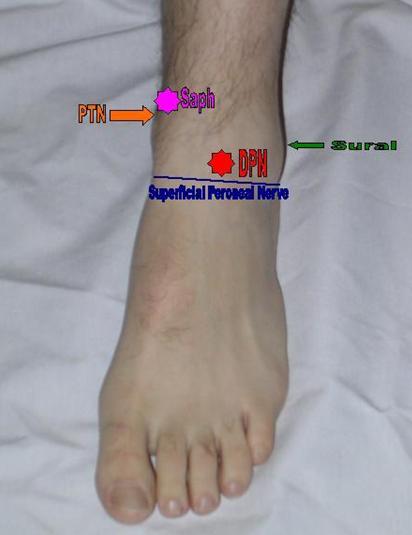
Areas of anesthetization to complete an ankle block. This block requires anesthetization of 5 nerves for complete sensory block below the ankle. The areas to anesthetize include a line along the anterior ankle for the superficial peroneal nerve (blue line), the deep peroneal nerve (red star), the saphenous nerve (pink star), the sural nerve (green arrow), and the posterior tibial nerve (orange arrow).
- Incision and drainage of an abscess in the dorsal regions of the foot
- Removal of foreign body in the dorsal regions of the foot
- Toenail repair (Toenail repair on the lateral first digit and medial second digit also requires deep peroneal nerve block.)
- Symptomatic relief of compression of the common peroneal nerve (along with the deep peroneal nerve block)
Contraindications
- Allergy to anesthetic solution or additives (eg, ester, amide)
- Overlying cellulitis
- Severe bleeding disorder or coagulopathy
- Preexisting neurological damage
- Patient uncooperativeness (Pediatric or elderly patients may need sedation.)
Anesthesia
- Lidocaine, the most commonly used anesthetic, has a fast onset of action and a duration of action of 30-120 minutes, which is increased to 60-400 minutes with the addition of epinephrine. The total cumulative dose of lidocaine to be infiltrated is 4.5-5 mg/kg (not to exceed 300 mg) if lidocaine without epinephrine is used, and 7 mg/kg (not to exceed 500 mg) if lidocaine with epinephrine is used.
- Topical anesthetics may be needed in children or uncooperative adults.
Equipment
- Needle, 4 cm, 25 gauge (ga)
- Needle, 18 ga
- Syringe, 10 mL
- Marking pen
- Sterile gloves
- Antiseptic solution (eg, povidone iodine [Betadine] or chlorhexidine gluconate [Hibiclens]) with skin swabs
- Alcohol swabs
- Sterile drape
- Lidocaine 1%, 10 mL
- Facial mask with eye shield
- Sterile gauze
Positioning
- Position the patient supine, with the ankle supported by a pillow or rolled sheet, optimizing comfort.
- Alternatively, the patient may sit and face the physician while maintaining a similar leg elevation.
Technique
- Explain the procedure, benefits, risks, and complications to the patient and/or patient’s representative, and inform the patient of the possibility of paresthesia during the procedure.
- Obtain informed consent in accordance with hospital protocol.
- Perform and document neurovascular and musculoskeletal examinations prior to the procedure. Testing the superficial peroneal nerve prior to performing the block includes the following:
- Sensation of dorsum of the foot
Superficial peroneal nerve dermatome at the level of the anterior lower leg.
- Foot eversion
- Expose the area of injection and identify the medial and lateral malleoli by palpation.
- Draw a line from the distal anterior aspect of the lateral malleolus to the anterior border of the medial malleolus.

Line of anesthesia from lateral malleolus to medial malleolus.
- Wipe the area with an alcohol pad and clean the site thoroughly with antiseptic solution, moving outward in a circular fashion.
- Maintaining sterile technique, place an initial skin wheal of lidocaine anterior to the distal lateral malleolus using a 25-ga needle.
- Insert the 25-ga needle through the skin wheal and infiltrate 6-10 mL in a transverse fashion until the medial malleolus is reached.

Anesthetize along the line from lateral to medial malleolus.
Pearls
- Equipment preparation and proper patient positioning may make the difference between success and failure.
- In children or noncompliant adults, consider using topical anesthetic mixtures, such as lidocaine, epinephrine, tetracaine (LET) or a eutectic mixture of lidocaine and prilocaine (EMLA cream).
- Pediatric or elderly patients may require additional sedation for compliance.
- Consider a hematoma block or bier block to attain more effective analgesia when a fracture exists or when more extensive manipulation of the foot is expected.
- Adding a buffering solution, like sodium bicarbonate, can significantly decrease the pain of the injection when performing a nerve block. Add 1 mL of sodium bicarbonate (44 mEq/50 mL) to 9 mL of lidocaine.
- Warming the anesthetic solution to body temperature can significantly decrease the pain of the injection.
- When unassisted, tape a bottle of lidocaine upside down to the wall prior to the procedure. If more anesthetic is needed during the procedure, it can be obtained from this bottle without compromising the sterility of gloves and equipment.
Complications
- Infection: Infection occurs when the puncture site is not clean. Avoid puncture through infected skin or skin lesions. Be sure to use sterile technique during the procedure, as the risk of infection is insignificant when sterility is properly maintained.
- Intravascular injection: Intra-arterial injection may result in vasospasm and lead to ischemia of the limb tissue. Intravenous injection can lead to systemic toxicity when high doses of anesthetic are injected. Tissue texture changes revealing pallor, bogginess, and cool temperature may indicate that either intravascular injection or vascular compression has occurred. Always aspirate the syringe to rule out intravascular placement before injection. Alpha-adrenergic antagonists (eg, phentolamine 0.5-5 mg diluted 1:1 with NaCl 0.9%) can be administered by local infiltration to relieve arterial vasospasm secondary to intra-arterial injection.
- Nerve injury: Patients may develop paresthesia, sensory deficits, or motor deficits secondary to inflammation of the nerve. Most often, this type of neuritis is transient and resolves completely. During the procedure, pull back gently after induction of paresthesia so as to not inject the nerve directly. Make sure to document a complete neuromuscular examination both before and after the procedure.
- Hemorrhage: Reports of significant hemorrhage during regional anesthesia are rare, even in patients who have blood coagulopathies. A hematoma may develop with intravascular puncture. If prolonged bleeding occurs, attempt to obtain hemostasis with direct pressure and elevation.
- Allergic reaction: Allergic reactions to local anesthetics occur at a rate of 1%. Reactions range from delayed hypersensitivity (type IV) to anaphylactic (type I). Although rare, the most common cause of such an allergic reaction is the preservative (eg, methylparaben) in the local anesthetic solution. Preservative-free lidocaine (typically found in cardiac solutions) is an alternative, since it does not contain the preservative. Alternatively, a 1-2% diphenhydramine solution can be used as a local anesthetic.
- Exceeding total dose of anesthesia: The dose of 1% lidocaine without epinephrine should not exceed 5 mg/kg. If lidocaine with epinephrine is used, total dose should not exceed 7 mg/kg. Systemic toxicity manifests in the central nervous and cardiovascular systems. Signs such as tremors, convulsions, tachycardia, or respiratory compromise should alert the physician to stop the procedure and reassess the patient.
Ultrasonographic Guidance
A disadvantage of the ankle block is that it usually requires large volumes of local anesthetic. According to Frederickson, these volumes can be reduced with the use of ultrasonographic guidance because of the more precise needle placement and real-time repositioning that such guidance allows. This refernce paper states that typical volumes of 30 mL can be reduced to 15 mL for the entire ankle block.
Four of the five nerves in the ankle block can be approached with an in-plane needle transducer orientation directly, using a vessel as a guide, except for the superficial peronieal nerve. These nerves and their corresponding vessels are as follows:
- Deep peroneal nerve – Lateral to anterior tibial artery
- Posterior tibial nerve – Posterior to posterior tibial artery
- Saphenous nerve – Adjacent to the long saphenous vein
- Sural nerve – Adjacent to the short saphenous vein
As noted by Frederickson, the superficial peroneal nerve is approaced in a traditional manner, as it does not travel with a vessel.
Source Emedicine.medscape.com
(Lưu ý: Việc đáp ứng với các liệu trình điều trị, máy, thiết bị trợ giúp là khác nhau tùy thuộc cơ địa mỗi người !
Những thông tin y học trên website chỉ mang tính tham khảo, bạn không được tự ý áp dụng nếu chưa được sự chỉ dẫn của thầy thuốc !)

