For the assessment of shoulder instability and labral tears, it is imperative that intra-articular contrast medium be injected in order to be able to evaluate the entire articular labrum, glenoid fossa, and capsular mechanism (12). Axial MR images provide the best visualization of the anterior and posterior glenoid labra, capsule, and lower rotator cuff muscles (Fig. 6-1). Anteriorly, the moderate–signal-intensity subscapularis muscle belly and its low–signal-intensity tendon are visualized. The tendon fuses with the low–signal-intensity anterior capsule as it courses to its insertion on the lesser tubercle. The fibrocartilaginous anterior and posterior labra appear as low–signal-intensity triangular or rounded areas attached to the glenoid rim. The higher–signalintensity intra-articular contrast opposed the hyaline cartilage surfaces of the glenoid and humeral head. The posterior capsule is visualized as a low-intensity area blending with the deep surface of infraspinatus and teres minor muscles as they extend to their insertions on the greater tubercle of the humerus. The long tendon of the biceps is demonstrated as a round, low– signal-intensity area within the bicipital groove.
Shoulder instability and the associated disruption of the anterior capsular mechanism can cause chronic shoulder pain and disability. The instability may be caused by an acute traumatic
episode or can occur with no history of a traumatic event. Both recurrent traumatic subluxation and nontraumatic instability are typically associated with disruption of the anterior capsular mechanism. Anteriorly, where most instability occurs, this mechanism includes the subscapularis muscle and tendon, the anterior joint capsule, three underlying glenohumeral ligaments, the synovial lining, and the anterior labrum. With instability, the labrum shows tears, separation from the glenoid rim, or degeneration (13). Also frequently present are medial stripping of the capsule from its normal attachment to the labrum and glenoid rim, an enlarged fluid-filled subscapular bursa secondary to joint effusion, attenuation of the glenohumeral ligaments, and injury or laxity of the subscapularis muscle or tendon.
By MRI, labral tears may be visualized as discrete linear areas of increased signal intensity within the normal signal void of the labrum (Figs. 6-6 and 6-7). These areas show moderate intensity on T1-weighted images and high intensity on T2-weighted images. With recurrent dislocation or subluxation, the labrum can become fragmented or attenuated.
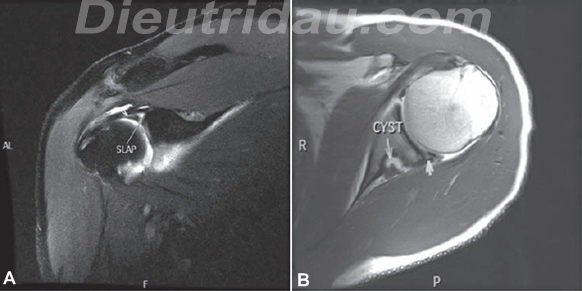
FIGURE 6-6. SLAP lesion and posterior labral tear in a patient with history of posterior instability. A: Coronal oblique T1-weighted fat suppressed MR arthrogram demonstrates increased signal intensity within the BLC extending on the biceps tendon (arrowhead) characteristic of a type IV SLAP lesion. B: Axial T1-weighted MR arthrogram demonstrates increased signal within the posterior labrum (arrowhead ). There is a cyst within the posterior aspect of the spinoglenoid notch with high–signal-intensity contrast extending into the cyst.

FIGURE 6-7. Bankart lesion. A: Axial T1-weighted images of a left shoulder MR arthrogram demonstrate the fibrocartilaginous Bankart lesion of the anterior glenoid labrum (arrow). B: Coronal T1-weighted fat suppression demonstrates the inferior (short arrow) and the superior (long arrow) extensions of the labral tears.
Capsular detachment from the scapula (i.e., stripping) is visualized by T2-weighted MRI as an area of high–signalintensity fluid dissecting medially from the glenoid rim. With trauma to the subscapularis tendon, there can be medial retraction of the muscle-tendon junction when the tendon is completely ruptured. Chronic atrophy of the subscapularis muscle belly is identified by high–signal-intensity fatty replacement. The glenoid marrow underlying a labral detachment may show pathologically decreased signal intensity even before the plain film radiograph shows an osseous Bankart lesion. MRI and CT can be used to visualize Bankart fractures of the anterior glenoid and the Hill-Sachs compression deformity of the posterolateral humeral head (14,15) and are both useful in the assessment of the extent of a Hill-Sachs defect in patients with engaging lesions. Patients with the rarer posterior instability show similar posterior labral, capsular, and muscular defects.
Source: Physical Medicine and Rehabilitation – Principles and Practice
(Lưu ý: Việc đáp ứng với các liệu trình điều trị, máy, thiết bị trợ giúp là khác nhau tùy thuộc cơ địa mỗi người !
Những thông tin y học trên website chỉ mang tính tham khảo, bạn không được tự ý áp dụng nếu chưa được sự chỉ dẫn của thầy thuốc !)

