General
Trigger points may occur in any muscle or muscle group of the body. They are commonly found in muscle groups that are routinely overstressed or those that do not undergo full contraction and relaxation cycles. Many trigger points are characterized by pain originating from small circumscribed areas of local hyperirritability involving myofascial structures, resulting in local and referred pain. Pain is aggravated by stretching, cooling, and compression of the affected area, which often gives rise to a characteristic pattern of referred pain (11,12).
Trigger points are best localized by deep palpation of the affected muscle, which reproduces the patient’s pain complaint both locally and in the referred zone. Trigger points are usually a sharply circumscribed spot of exquisite tenderness when they are present; passive or active stretching of the affected muscle routinely increases the pain. When compared with equivalent palpation pressure in normal muscle, the trigger point region displays isolated bands, increased tenderness, and referred pain. The muscle in the immediate vicinity of the trigger point is often described as ropey, tense, or a palpable band. The trigger point is injected after palpation of the affected muscle, and the point of maximal tenderness reproducing the pain complaint is identified. When the point of injection has been determined, it is best marked with the tip of a retracted ballpoint pen or needle hub by pressing the skin to reproduce temporary indentation to mark the point of entry. The patient is prepared in a standard aseptic fashion over an area large is used throughout the procedure. The skin and subcutaneous tissue at the injection site are usually not anesthetized. A 1½- to 2-in. (4- to 5-cm), 22- to 25-gauge needle is advanced into the muscle at the point of maximum tenderness. Before injecting the medication, an attempt should always be made to aspirate to avoid accidental or intravascular injection. Verification that the needle is at the trigger point may be established by the jump sign or reproduction of the pain complaint. Medication should be injected in a fanwise manner in the area of the trigger point.
Indications for Trigger Point Injections
Trigger point injections may be used to determine the source of pain and to provide maximum pain relief from myofascial pain and to facilitate physical therapy for the stretching of trigger points.
Contraindications for Trigger Point Injections
Absolute contraindications to trigger point injection include localized infection, a skin condition that prevents adequate skin preparation, the existence of a tumor at the injection site, history of allergy to local anesthetics, gross coagulation defects, septicemia, or an uncooperative patient.
Complications
The complications associated with trigger point injections include infection, increased pain, local anesthetic overdose, or intravascular injection that can result in CNS toxicity and, in some cases, pulmonary and cardiac arrest. Intraneural injection may result in nerve damage. Severe pain on injection suggests the possibility of an intraneural injection, and the needle should be immediately repositioned. Other complications depend on location of the trigger point injection and are discussed separately.
Techniques
Before the injection, the affected muscle is palpated and the trigger points located and marked. The skin is scrubbed with antiseptic and allowed to dry for 2 minutes. The wearing of sterile gloves is required so that muscle in the sterile field may be palpated throughout the procedure. Before the injection, the trigger point is repalpated and stabilized between the fingers for injection (Fig. 67-20). Routinely, a 1½-in. (4-cm), 21- to 25-gauge needle transverses the skin’s subcutaneous tissue and is advanced smoothly into the area of the trigger point.
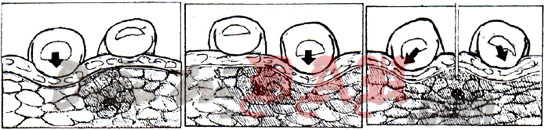
FIGURE 67-20. Trigger point palpation. A, B: Palpation and localization of trigger point by rolling beneath two fingers (arrows). C: Stabilization of trigger point for injection by spanning with two fingers (arrows).
Aspiration should be done to ensure there is no intravascular penetration. If this does occur, the needle should be repositioned and aspirated to ensure that blood vessels have been avoided, and then the medication is injected. A fanwise manner of injection often results in the longest pain relief, owing to increased distribution of local anesthetic (Fig. 67-21). The needle is then withdrawn, with pressure applied to minimize bleeding.

FIGURE 67-21. Fanwise injection technique for trigger point.
Source: Physical Medicine and Rehabilitation – Principles and Practice
(Lưu ý: Việc đáp ứng với các liệu trình điều trị, máy, thiết bị trợ giúp là khác nhau tùy thuộc cơ địa mỗi người !
Những thông tin y học trên website chỉ mang tính tham khảo, bạn không được tự ý áp dụng nếu chưa được sự chỉ dẫn của thầy thuốc !)

